Use this index to navigate to MuscleCare Product Information
MuscleCare’s product range comprises three unique formulations—Cold Gel, Ointment, and Massage Lotion. Each of the products have some features in common:

MuscleCare Extra Strength Roll on (retail) and Cold Gel(back bar or in clinic) – 16 ingredients
Main Benefits
Additional DC and PT Notes
Main Features
Additional DC and PT Notes:
Main Features
Additional DC and PT Notes
These pump quantities reflect real-world usage.
| Product | Purpose | DC Use | Approx. Cost to clinic |
|---|---|---|---|
| Massage Lotion | Base layer for full-area work | 2–4 pumps | $0.36–$0.72 |
| Ointment | Focused treatment on trouble spots | Up to 2 pumps | $0.32 |
| Cold Gel | Cooling effect, post-session focus | Up to 2 pumps | $0.28 |
MuscleCare outperforms Biofreeze in two critical ways: it’s clinically proven to deliver greater pain relief, and it uses a cleaner, safer formulation — key reasons why major chains have chosen to make the switch.
Cleaner Formulation
MuscleCare is free of parabens, dyes, and harsh chemicals commonly found in other products. We understand the concerns surrounding ingredients that are in Biofreeze – to name a few:
‘In-clinic’ protocols are below for DC’s, PT’s and LMTs.
Step 1
Use MuscleCare Massage Lotion to prepare the superficial and middle layer tissues Identify the location of the most contracted muscles.
Step 2
Use MuscleCare Pain Relieving Ointment to target the stiff tissues
Step 3
Use MuscleCare Pain Relieving Cold Gel to target inflammation or acute pain
MuscleCare’s SmartQR:
This QR code is on every product. Customers can scan the code to be directed to pain specific stretch, ergonomic, and protocols on product use.

MuscleCare is a professional-grade, root-cause sub-topical, over-the-counter (OTC) topical pain relief product designed to enhance therapeutic soft tissue care sessions through targeted relief of tension, inflammation, and discomfort.
MuscleCare for DCs, LMTs, and PTs: Here's what matters most to you:
MuscleCare has been clinically proven to offer significantly superior pain relief compared to major national brand pain brands such as biofreeze, IcyHot, and Placebo as well as equal to or slightly greater than NSAID creams Voltaren, while MuscleCare only contains natural ingredients.
In a randomized, double-blind study involving 120 participants, MuscleCare outperformed four top national brands and placebo, demonstrating faster and more effective pain relief. View Details
Additionally, a 2017 University of Toronto study led by Dr. Jack Goodman found that MuscleCare was equal to, and in some cases slightly more effective than, diclofenac-based creams such as Voltaren, suggesting its potential to become the preferred recommendation for acute pain among physicians. View Details
Beyond its effectiveness, MuscleCare has also been validated as safe for use during pregnancy and breastfeeding, according to research conducted by Motherisk at Sick Children’s Hospital, University of Toronto, making it a rare over-the-counter option suitable for these sensitive populations. View Details
We recommend that this 60 second tool be sent to all of your clinic team members and to all of your patients, allowing them to have a visual understanding of the innovation you have brought to their care.
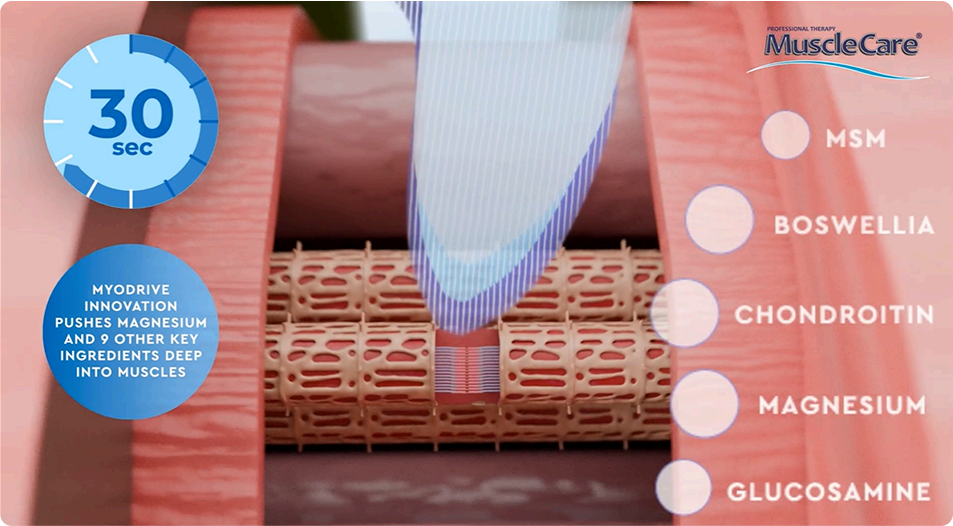
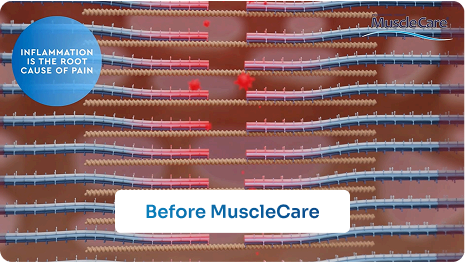
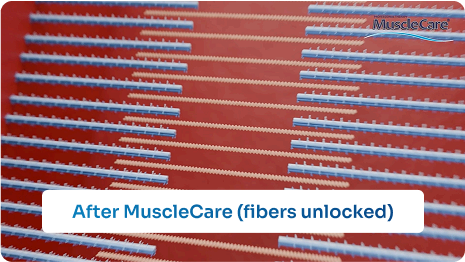
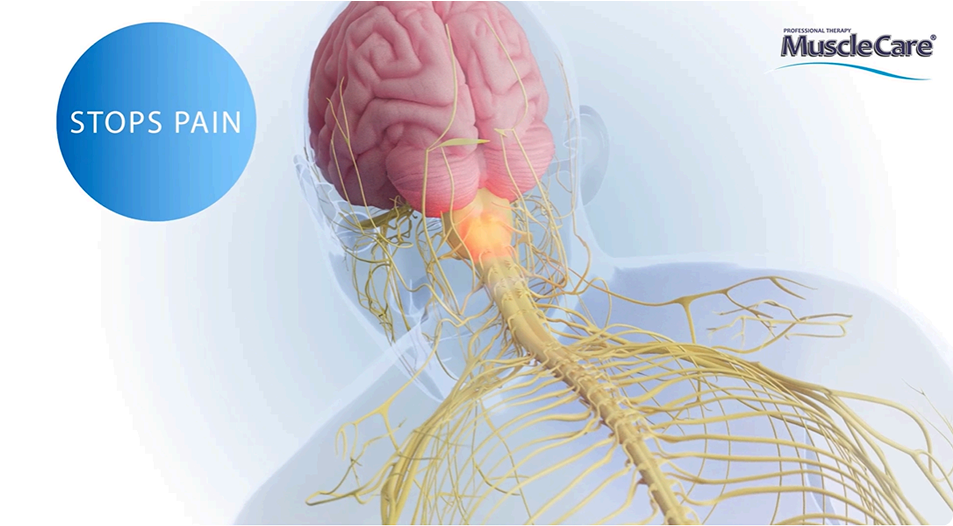
This short training video explains the science behind MuscleCare’s effectiveness in reducing muscle pain, inflammation and tension. It walks you through MyoDrive, a patented transdermal delivery system that helps key ingredients penetrate the skin deeper to elicit their effect sub-topically. Dr. Urquart ( molecular biologist) explains that when muscle fibers are locked due to injury or insult, pain signals are excited to the brain, where by relaxing muscles you improve local circulation and help flush out metabolic waste that contributes to inflammation thus causing pain. Using clear visuals, the video shows step-by-step how MuscleCare doesn’t merely rely on cooling or heating, masking the symptoms, but is designed to target the root causes of discomfort. — making it a powerful tool you can integrate into client care to enhance soft tissue therapy outcomes and provide lasting relief.
Combination of natural, nourishing ingredients enhances dermal penetration of actives that can move efficiently into underlying muscle tissue rather than remaining on the skin surface.
Takeaway: This means as you rub in MuscleCare, MyoDrive’s skin penetration ingredients are aiding Magnesium to unlock muscle fibers, the source of our pain and making the soft tissue therapy less physical effort for the thus designed to reduce burn out.
Science: MuscleCare uses a patented MyoDrive™ delivery system, the unique
Science: Once absorbed, the relaxation of muscles increases local circulation and reduces inflammation. The animation shows improved oxygen flow and removal of metabolic waste by natural existing nutrient laden circulation.
Takeaway: This is why clients feel more than just a cooling/warming sensation—Magnesium, the key ingredient in MuscleCare, changes the muscle physiology.
Science: Peer-reviewed, published studies show MuscleCare offers significantly greater( pressure pain tolerance) pain relief than biofreeze, insignificantly greater than NSAIDs, while being 100% natural!
Takeaway: This is not a “surface-level rub”; it’s evidence-based relief that complements your manual therapy. This is a natural root cause sub-topical.
Here are the 4 talking points for explaining the key points of MuscleCare to your clients
MuscleCare is ideal for both relief and relaxation because it targets the underlying muscle tension that often causes discomfort, even in clients who come in simply to unwind. Many people experience stiffness or mild soreness they may not mention, and MuscleCare helps address that quickly and effectively. Therapists note Its fast-acting formula softens tissue, has an improved glide, and enhances the overall soft tissue experience without leaving behind a strong scent or residue. This makes it a practical and versatile tool for delivering both therapeutic results and a more relaxing session.
Key Facts:
Dr. Chris Oswald is a seasoned chiropractor with 37 years of clinical experience and the founder of Canada’s largest multidisciplinary pain clinic, The Centre for Fitness, Health and Performance and The Jaw centre. Over the course of his career, he personally treated more than 30,000 new patients, which gave him deep insight into the limitations and risks of conventional pain relief treatments. He recognized a major gap in the market: the need for a safe, effective, and side-effect-free solution that could be used across all age groups and conditions. This realization drove him to create MuscleCare, a natural, root-cause-focused sub-topical pain reliever designed to treat spasms, inflammation, and pain without relying on harsh chemicals or drugs. His Jaw centre, in Toronto, has an 800 dentist referral base responsible for 260 New Patients per month.
Determined to prove its effectiveness, Dr. Chris led MuscleCare through rigorous third-party clinical testing, including double-blind, randomized controlled studies. These studies showed that MuscleCare outperformed leading national pain relief brands, and was found to be slightly more effective than NSAID creams containing diclofenac, such as Voltaren. Further testing by the University of Toronto and approval by Sick Children’s Hospital validated its safety for even the most vulnerable users. Dr. Chris’s vision was to create a trusted, professional-grade solution that could transform the standard of pain relief in North America, making it both safer and more accessible for the millions suffering from musculoskeletal pain.

All MuscleCare products have a QR code on the side of the packet. This code sends the user to our ‘My Pain University’, where they can find focused, pain-type stretches to use at home (with MuscleCare ideally, to maximize the impact) and maximize their rehabilitation.
Two products are available for retail:
Products Available: ( these items are not sold on Amazon or mass retail)
The deepest penetrating product – ideal for longer lasting or chronic issues, like arthritis, Fibromyalgia or past whiplash. Has a mild cooling sensation and wintergreen smell.
The strongest all-natural, scientifically based, topical analgesic, anti-inflammatory, and anti-spasmodic otc product available. combining menthol and camphor for immediate pain relief with magnesium, glucosamine, MSM, and chondroitin to relax muscle tension, improve circulation, and reset the muscle in its normal resting state.
Answer: MuscleCare is the only all-natural, root-cause, sub-topical pain relief formula backed by clinical studies
and powered by a proprietary delivery system called MyoDrive™. Unlike most topical products (like
Biofreeze or Icy Hot) that work as counterirritants by masking pain with cold or heat, MuscleCare works
at the muscular level. It:
Answer: No, and this is a common misconception. While both are topicals used in therapy, they function very differently:
| Feature | Biofreeze | MuscleCare |
|---|---|---|
| Action | Surface-level cold therapy | Deep-tissue muscle fiber release |
| Type | Counterirritant | Sub-topical root cause muscle /joint therapy- patented MyoDrive Technology |
| Duration | Short-acting | Lasts 6+ hours |
| Key Ingredients | Menthol | Magnesium, MSM, Glucosamine, 16 in total, etc. |
| Clinical Studies | Zero clinical studies, minimal comparative data | Outperformed Biofreeze in RCTs, two RCTS and Sick Children’s hospital study reporting safe to use in pregnancy pain |
| Use for all cohorts | Not advised | Clinically proven safe for all |
MuscleCare is designed for therapeutic function, not just temporary sensory relief.
Answer: Magnesium is a critical mineral for muscle function—it helps regulate muscle contraction and relaxation, reduce nerve excitability, and ease muscle cramps and spasms. In MuscleCare, topically applied magnesium (delivered via MyoDrive™) penetrates to relax tense or locked muscles quickly, making your job easier and more effective. Magnesium works with ATP and blocks calcium channels allowing the release of the actin and myosin cross bridges that maintained the tension, spasm or cramp.
Magnesium is one of the key reasons MuscleCare works so fast without needing heat, cold, or manual friction.
Answer: NO! Not necessarily— we do recommend that the Massage Lotion is used first followed by the Ointment. The cold gel is not a must. If a patient doesn’t like cold or it is cold outside, avoid it. If there is still discomfort and or inflammation we recommend using the cold gel. Note, using them all together enhances results:
You can customize your approach based on the client’s condition and treatment goals. Many DCs find value in having all three available.
Answer: Yes — and that’s a great clinical strategy.
Start by applying the Cold Gel 1–3 times over a few minutes to reduce acute pain, irritation, or hypertonicity. Once the tissue has settled, follow with the Ointment for deeper muscle engagement and longer-lasting relief.
This combo lets you work more effectively with less resistance, particularly with new clients, post-injury recovery, or inflamed tissue.
Answer: Yes, that’s normal and harmless—and actually a sign that the skin is detoxifying and shedding dead cells. The Cold Gel contains natural actives and delivery agents that can gently exfoliate the skin during soft tissue care, especially in areas with dry skin or product buildup. This is why we suggest the cold gel be wiped with one pass over a painful area, allowed to absorb and then the client is sent home. The notion of massaging with cold gel is when a very acute state exists and you start with one pass, allow absorption and then another pump with gentle soft tissue techniques.
You can reassure clients this is temporary, healthy, and non-irritating—and it won’t affect the effectiveness of the product.
Answer: You don’t need MuscleCare to be a great DC—but it can help you become an even more effective and efficient one, while helping your hands and arms feel less strain. This is why Dr Chris developed Musclecare to save his hands and thumbs;
Here’s why:
You’re still the expert—but MuscleCare helps you do more, faster, and with better client satisfaction.
Answer: Yes — MuscleCare roll on is fully compatible with RockTape and all kinesiology taping methods. Tape first and use roll on or cold gel on top of the tape for best therapeutic benefit.
In fact, it’s a perfect complement. Here’s how to integrate them effectively:
By magnesium unlocking muscle fibers, tissue function, circulation, and relaxation are improved. These conditions allow the neuromuscular feedback of RockTape to be even more effective. Together, MuscleCare and RockTape could create a synergistic treatment experience that supports longer-lasting relief, better posture, and faster recovery.
Answer: Yes — MuscleCare and CBD can safely be used together, and in many cases, they complement each other without conflict. Avoid CBD in pregnancy.
While both offer pain relief, they work through different mechanisms:
| Ingredient | Primary Action | Notes |
| MuscleCare | Unlocks muscle fibers, which boosts circulation, and flushes inflammatory chemicals | Fast-acting, mechanical and biochemical relief |
| CBD | Acts on the endocannabinoid system to reduce pain signaling and inflammation | Slower onset, works neurologically. Masks symptoms, doesn’t aid in repair |
How to use them together:
This section outlines key musculoskeletal pain contributors by region, with a focus on the most commonly affected muscles and the clinical impact of soft tissue therapy. For each area, evidence-based insights are provided to highlight how specific manual techniques—such as myofascial release, trigger point therapy, or transverse friction soft tissue therapy—can reduce pain, improve range of motion, and support functional recovery. Where applicable, supporting studies from randomized controlled trials are included to guide best practices and reinforce therapeutic decision-making.
Dr Chris’ Guidelines include training for maximizing your care in these areas:
Dr Chris suggests following this video for how best to provide soft tissue therapy to the Lower Back when addressing pain in the area.
Muscles Involved (main pain contributors)
Soft tissue therapy Impact on Pain at these Muscles supported by scientific published studies.
Quadratus lumborum
Erector spinae (lumbar paraspinals)
Dr Chris suggests following this video for how best to address the Neck when addressing pain in the area.
Muscles Involved (main pain contributors)
Upper Trapezius
Soft tissue Impact on Pain at these Muscles
Sternocleidomastoid (SCM) & Splenius Group/ SCM and Scalene tissues often are blended together anatomically;
Dr Chris suggests following this video for how best to perform soft tissue therapy on the shoulder when addressing pain in the area
Muscles Involved (main pain contributors)
Other muscles such as the upper trapezius, infraspinatus, deltoid, and biceps may be indirectly referenced based on myofascial trigger points in broader studies—but the focal RCT referenced below targets supraspinatus explicitly. An understanding of the brachial plexus anatomy and the manner with which these nerves pass through the scalene tissue force us to focus on the scalene tissues in soft tissue therapy.
Soft tissue Impact on Pain at these Muscles
Supraspinatus (Ischemic Compression of Trigger Points in Shoulder Muscles)
Dr Chris suggests following this video for how best to use soft tissue therapy on the Elbow when addressing pain in the area.
Extensor Carpi Radialis Brevis (ECRB)
Brachioradialis
Soft tissue Impact on Pain at these Muscles
Extensor Carpi Radialis Brevis (ECRB)
Brachioradialis
Systemic Pain Area Clinical Pearls and Recommended Treatment Guidelines
Systemic Pain Area Treatment Reviews and Clinical Pearls
This section outlines key musculoskeletal pain contributors by region, with a focus on the most commonly affected muscles and the clinical impact of massage therapy. For each area, evidence-based insights are provided to highlight how specific manual techniques—such as myofascial release, trigger point therapy, or transverse friction massage—can reduce pain, improve range of motion, and support functional recovery. Where applicable, supporting studies from randomized controlled trials are included to guide best practices and reinforce therapeutic decision-making.
In this Knee and Foot Clinical Pearls video, Dr. Chris Oswald offers a comprehensive overview of how foot dysfunction, particularly overpronation, impacts the entire lower kinetic chain, from the arches to the knees, hips, and lower back. He emphasizes the importance of assessing footwear, foot structure, and soft tissue imbalances, while demonstrating how to integrate chiropractic adjustments, orthotic support, and targeted use of MuscleCare Maximum Strength Ointment and Roll-On for conditions like plantar fasciitis, sesamoiditis, Morton’s neuroma, shin splints, and patellar tracking issues. Dr. Oswald provides clinical insights into specific muscles and joint structures—including the navicular, calcaneus, tibia, popliteus, and patella—and explains manual techniques and treatment protocols aimed at reducing inflammation, improving alignment, and restoring functional movement. The session is designed to guide LMTs in delivering more effective, evidence-informed care using both manual therapy and topical support.
(We break down the our muscle assessment into both groups here, Feet and Knee)
Muscles Involved (main pain contributors)
Massage Impact on Pain at these Muscles
Soleus
Flexor digitorum brevis
Muscles Involved (main pain contributors)
Massage Impact on Pain at these Muscles
Quadriceps
In this Clinical Pearl video, Dr. Chris Oswald, founder of MuscleCare and a chiropractor with 37 years of experience, shares expert insight into treating forearm, wrist, and hand problems — including carpal tunnel syndrome. He explains how these issues are often rooted in tight forearm muscles, poor gliding surfaces, and fascial adhesions. Dr. Oswald demonstrates a practical, clinic-ready approach using MuscleCare topicals with manual techniques, showing how to assess, treat, and restore mobility and nerve function. He also covers how to combine MuscleCare with tools like ultrasound and shockwave therapy to maximize penetration and effectiveness, all while keeping ingredients clean, therapeutic, and natural.
Muscles Involved (main pain contributors)
Massage Impact on Pain at this Muscle
Pronator teres
In this Low Back Pain Clinical Pearls video, Dr. Chris Oswald presents a concise, evidence-informed approach to assessing and treating mechanical low back pain by addressing segmental restrictions, pelvic instability, and soft tissue dysfunction in muscles like the QL, psoas, and glute medius. He demonstrates how to integrate chiropractic adjustments, neuromuscular activation, and manual therapy with the targeted use of MuscleCare Maximum Strength Ointment and Roll-On to accelerate tissue release, reduce therapist effort, and extend pain relief. The ointment is used pre-treatment to relax tissue and improve adjustment outcomes, while the Roll-On supports post-treatment recovery and home care. Dr. Oswald emphasizes MuscleCare’s ability to treat the root cause of pain—muscle tension and inflammation—rather than masking symptoms, highlighting its clinically proven efficacy over BioFreeze, Icy Hot, and Voltaren, and its safety for all patients, including those who are pregnant or breastfeeding.
Muscles Involved (main pain contributors)
Massage Impact on Pain at these Muscles
Quadratus lumborum
Erector spinae (lumbar paraspinals)
In this Upper Cervical Syndrome Clinical Pearls video, Dr. Chris Oswald explores the complex relationship between forward head posture, chronic neck tension, and symptoms like headaches, jaw pain, and insomnia. Drawing on 37 years of experience, he explains how modern postural habits—particularly tech-induced anterior head carriage—create excessive contraction in posterior suboccipital tissues and anterior structures like the SCMs and scalenes, leading to mechanical dysfunction. While upper cervical adjustments (C1/C2) remain effective, Dr. Oswald emphasizes they are insufficient alone. He recommends first releasing soft tissue tension using MuscleCare Maximum Strength Ointment to relax 60–70% of contraction before adjusting, improving precision and outcomes. For patients with longstanding poor ergonomics, he advises sending them home with the retail ointment and educating them to scan the QR code for home stretching protocols. For more superficial or mid-level issues, especially in workplace settings, the Roll-On is ideal for mess-free application to both the front and back of the neck. Combining anterior and posterior adjustments with targeted soft tissue work and MuscleCare ensures optimal realignment, symptom relief, and long-term patient empowerment.
Muscles Involved (main pain contributors)
Massage Impact on Pain at these Muscles
Suboccipitals
Upper trapezius
In this Upper Thoracic Syndrome Clinical Pearls video, Dr. Chris Oswald addresses the widespread postural strain caused by chronic forward head positioning and tech use, particularly at the C7–T1–T2 junction. He explains how sustained cervical flexion accelerates disc degeneration and activates the sympathetic nervous system at the T1 level, contributing to anxiety, pain, and numbness. Dr. Oswald emphasizes the importance of correcting posture through anterior thoracic adjustments and soft tissue release, especially of the SCMs, scalenes, trapezius, and rhomboids. To enhance treatment, he recommends using MuscleCare Maximum Strength Ointment to release adhesions pre-adjustment, and Cold Gel for acute presentations due to its rapid MyoDrive delivery and muscle relaxation in under 30 seconds. He also highlights the importance of sending patients home with MuscleCare retail products, guiding them to the QR code on every bottle that offers free access to condition-specific stretches and protocols—reducing the need for repeated in-office education. Chronic cases benefit from the ointment applied morning and night, while the Roll-On is ideal for ongoing maintenance and occupational use. Dr. Oswald stresses that this integrated approach not only enhances outcomes but keeps patients functioning between visits, reducing acute flare-ups and clinic inefficiencies.
Muscles Involved (main pain contributors)
Massage Impact on Pain at this Muscle
Rhomboid major